by Gillian Hooker, PhD, CGC
Last week, at the Annual Education Conference of the National Society of Genetic Counselors, I shared data from an analysis in which we estimate the impact that proposed FDA regulation on laboratory developed tests (LDTs) will have on the genetic testing industry.
We see great value in data-driven stakeholder dialog throughout the regulatory process. We know that regulatory agencies do, too, especially given the complexity and pace of the precision medicine revolution and the broad desire to maintain and promote patient access to these new clinical tools while also maintaining safety.
The reason we’re sharing it on the blog is that, to our great delight, we had a good response to the talk and many participants asked that we do so.
For background, as we’ve discussed previously on the blog, LDT’s have been regulated since 1976 under the Center for Medicare and Medicaid Services (CMS) CLIA guidelines, which regulate how laboratories ensure quality processes are in place for testing. As such, the vast majority of new molecular diagnostics have come to market under CLIA. The proposed regulations released last year by the FDA represent a significant shift.
Details on the FDA’s perspective on LDTs can be found here.
A link to the draft guidance is here.
In summary, the draft guidance includes:
-
Notification of all marketed tests, which means all testing products will need to be registered with the FDA.
-
Adverse event notification
-
Risk-based regulation and prioritization
-
Class III / High Risk (highest priority for regulation)
-
Class II / Moderate Risk
-
Class I / Low Risk (exempted from many regulatory requirements)
-
-
Rare disease exemption for infrequently ordered tests
It’s reasonable to assume higher-risk tests will be subject to greater scrutiny, and will therefore require more time and investment on the part of developers to shepherd through the process.
As readers will know, we track the market for genetic testing products through a rigorous and standardized process. As a result, we know there are currently more than 53,000 genetic testing products available on the market not including testing for infectious disease. Every day, on average, approximately 8-10 new testing products are introduced into the market. Clearly, regulation of genetic tests will be a big undertaking, and the specific way the FDA chooses to define “high risk” will have a major impact on the way this process plays out.
So, we conducted a study to:
-
Estimate the number of genetic tests potentially subject to regulation by the FDA.
-
Estimate the number of high-risk genetic tests.
-
Explore areas of high-complexity for the regulation of genetic tests.
In this table, we assess three potential scenarios (using data from October 2015) for how the FDA may choose to define Class III / High Risk tests. The FDA has already stated that certain tests will definitely fall into the Class III category, while others will be determined by advisory panels.
| Test Categories | Number of Tests | Percent of Genetic Testing Market | |
|---|---|---|---|
| High Risk Test Scenario 1 | Products similar in nature to those already regulated by the FDA:
• Class III kits & devices • Companion Diagnostics |
587 | 1.12% |
| High Risk Test Scenario 2 | • Companion Diagnostics
• Class III kits & devices • Tests that target one of the ACMG 56 genes • Panels that include tests targeting one of the ACMG 56 |
3452 | 6.58% |
| High Risk Test Scenario 3 | • Companion Diagnostics
• Class III kits & devices • Tests that target one of the ACMG 56 genes • Panels that include tests targeting one of the ACMG 56 • Pharmacogenomic Tests • Non Invasive Prenatal Tests (NIPTs) • All Oncology tests |
7568 | 14.43% |
Data from October 2015
As you can see, one major variable is whether the FDA chooses to include the ACMG 56 in its definition of high-risk tests. If so, for these genes alone, that would involve:
-
56 genes
-
121 laboratories
-
331 clinical categories of tests (we refer to these as “bins”)
-
3455 different single and panel testing products
One thing to note, if a test that is comparable to a companion diagnostic in methodology and genes is marketed, it will be regulated as a companion diagnostic test. Hence, all BRCA1 & BRCA2 tests are included in the companion diagnostic category because they are potential competitors to BRACAnalysisTM CDx test offered by Myriad.
As a next step, we considered a practical, yet complex, question related to the rare disease exemption: Do these exemptions apply only to single gene testing products, or do they apply to any panel testing products that include that gene?
For example, Barth Syndrome is a rare disease (~1/1,000,000) caused by a mutation in TAZ. Regulation would only involve 21 single gene tests, many of which might meet the rare disease exemption due to the rarity of the disorder. But it could also involve an additional 91 panel tests, which have much broader indications for testing:
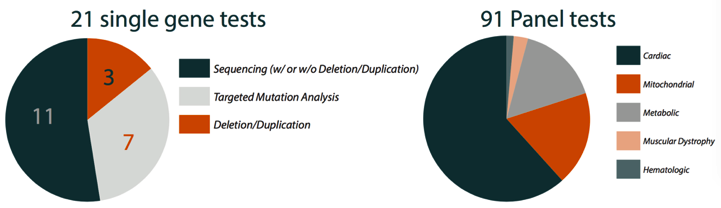
- Data from June 2015
So, this scenario raises interesting questions about how the rare disease exemption might be applied.
All of this leads us to a few conclusions:
-
The FDA’s decision to begin regulation (discontinue enforcement discretion) of LDTs stands to impact a large number of tests.
-
Input from the clinical genetics community, including genetic counselors, medical geneticists, medical laboratories and others, will be important in development of risk strata.
-
This challenge, however, provides a unique opportunity for innovative approaches to regulation that could provide benefits to all stakeholders.
One example of this type of innovation is the FDA’s work with DNAnexus to build precisionFDA, a research and development portal that will allow users to test, pilot, and validate existing and new bioinformatics approaches for processing Next Generation Sequencing (NGS).
We’re looking forward to continuing to watch this develop, recognizing the complexity of challenges facing both regulatory bodies and the industry as they work towards a common goal of improving genetics within clinical practice.
Finally, I’d like to acknowledge the work of my collaborators on this effort, including my colleagues Jud Schneider, PhD, Taylor Murphy, PhD, and Ashly Badgett, as well as R. Tanner Hagelstrom, PhD, from Munroe-Meyer Institute (http://www.unmc.edu/mmi/)